
The half-life of Mounjaro (tirzepatide) is approximately 5 days, a key pharmacokinetic property that enables its convenient once-weekly dosing schedule for adults with type 2 diabetes. Understanding this parameter helps patients and clinicians anticipate how long the medication remains active in the body, when steady-state concentrations are reached, and what to expect if treatment is interrupted or discontinued. This extended half-life, achieved through specific molecular modifications that enhance stability and albumin binding, distinguishes Mounjaro from shorter-acting diabetes medications and directly influences dosing intervals, missed-dose guidance, and the timeline for therapeutic effects.
Quick Answer: The half-life of Mounjaro (tirzepatide) is approximately 5 days, enabling once-weekly subcutaneous dosing for type 2 diabetes management.

Mounjaro® is the most innovative GLP-1 medication proven to dramatically curb appetite, hunger, and cravings to help professional men achieve substantial weight loss.
Start Here
Wegovy® is a weekly injectable GLP-1 medication with proven effectiveness in reducing appetite, hunger, and cravings to help busy professionals lose significant weight.
Start HereMounjaro (tirzepatide) is a prescription medicine licensed in the UK for the treatment of type 2 diabetes mellitus in adults. It is used as an adjunct to diet and exercise to improve glycaemic control, either as monotherapy when metformin is inappropriate or in combination with other diabetes medications. It is administered as a once-weekly subcutaneous injection and belongs to a novel class of medications that act as dual agonists, targeting both glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like peptide-1 (GLP-1) receptors. This dual mechanism distinguishes Mounjaro from other diabetes treatments and contributes to its efficacy in glycaemic control.
The mechanism of action involves stimulating insulin secretion from pancreatic beta cells in a glucose-dependent manner, meaning insulin is released only when blood glucose levels are elevated. This reduces the risk of hypoglycaemia compared to some other diabetes medications, although this risk increases when Mounjaro is used with sulfonylureas or insulin. Simultaneously, tirzepatide suppresses glucagon secretion from pancreatic alpha cells, which helps prevent the liver from producing excess glucose. Additionally, Mounjaro slows gastric emptying, which moderates the rate at which glucose enters the bloodstream after meals, and it acts on appetite centres in the brain to promote satiety and reduce food intake.
Clinical trials have demonstrated that Mounjaro can significantly reduce HbA1c levels (a measure of long-term blood glucose control) and promote substantial weight loss in many patients. The Medicines and Healthcare products Regulatory Agency (MHRA) has approved Mounjaro for use in adults with type 2 diabetes only; it is not indicated for type 1 diabetes or diabetic ketoacidosis. It is available in several dose strengths, allowing for gradual titration to optimise efficacy whilst minimising gastrointestinal side effects, which are among the most commonly reported adverse reactions. Suspected side effects should be reported via the MHRA Yellow Card Scheme at yellowcard.mhra.gov.uk or via the Yellow Card app.
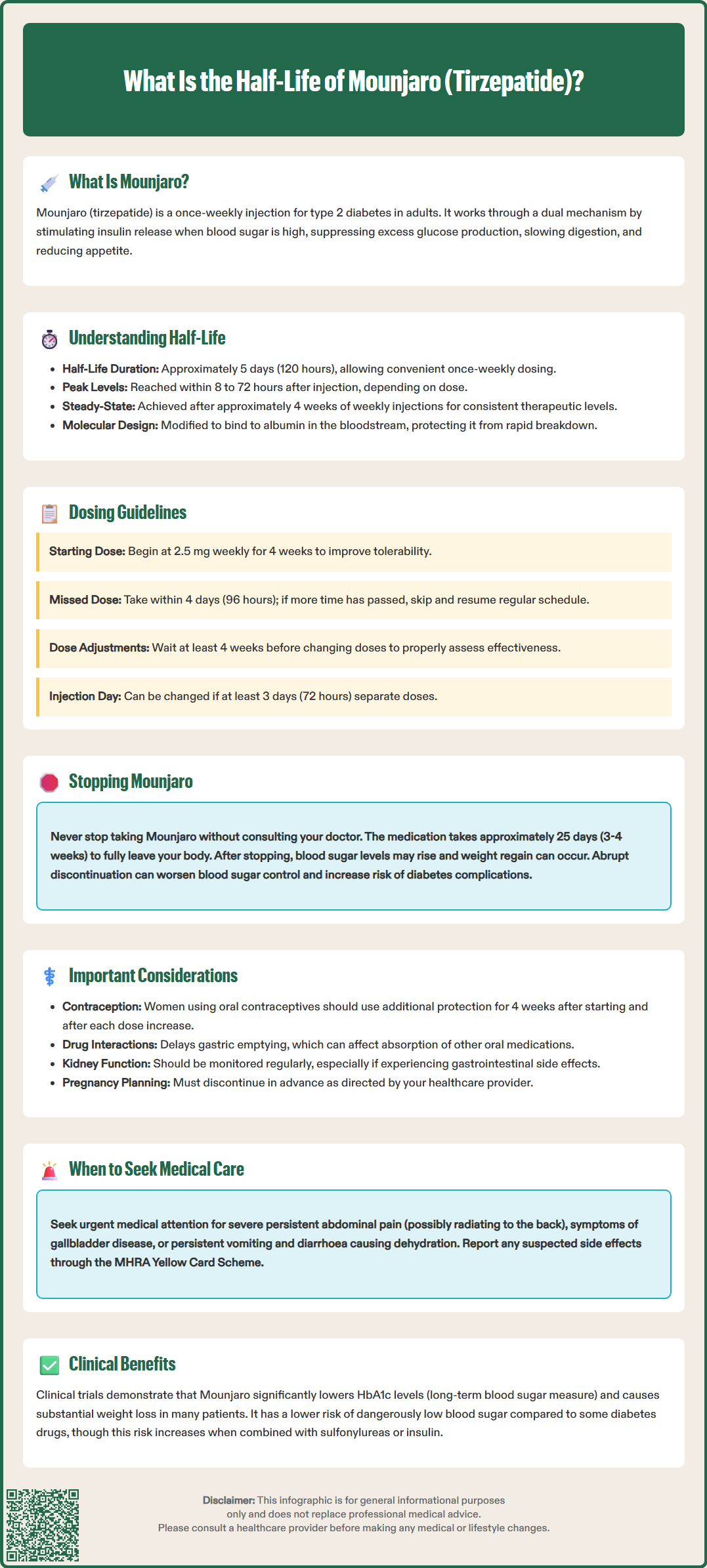
The half-life of a medication refers to the time it takes for the concentration of the drug in the bloodstream to reduce by half. Understanding this pharmacokinetic parameter is essential for determining appropriate dosing intervals and predicting how long a medicine remains active in the body. For Mounjaro (tirzepatide), the half-life is approximately 5 days (around 120 hours) following subcutaneous administration, according to the MHRA/EMC Summary of Product Characteristics (SmPC). This relatively long half-life is a key feature that enables once-weekly dosing, improving convenience and adherence for patients.
The extended half-life of tirzepatide is achieved through specific molecular modifications to the peptide structure. These modifications enhance the drug's stability and reduce its rate of degradation and elimination from the body. Tirzepatide binds to albumin in the bloodstream, which protects it from rapid enzymatic breakdown and renal clearance. This albumin binding is a deliberate design feature that prolongs the drug's duration of action and maintains therapeutic concentrations between doses.
After a single injection, tirzepatide reaches peak plasma concentrations within 8 to 72 hours, depending on the dose administered. Following repeated weekly injections, steady-state concentrations—where the amount of drug entering the body equals the amount being eliminated—are typically achieved after approximately 4 weeks of treatment. At steady state, the drug maintains consistent therapeutic levels, which is important for sustained glycaemic control and metabolic effects. It is worth noting that individual pharmacokinetic parameters may vary based on patient-specific factors, though the overall half-life remains relatively consistent across the population studied in clinical trials.
The 5-day half-life of Mounjaro directly informs its once-weekly dosing schedule, which is a significant advantage for patient convenience and treatment adherence. Because the drug remains in the body for an extended period, patients do not need to remember daily injections, reducing the treatment burden associated with diabetes management. The recommended starting dose is 2.5 mg once weekly for 4 weeks, which is primarily for improving gastrointestinal tolerability rather than achieving optimal glycaemic control. The dose is then gradually increased every 4 weeks based on glycaemic response and tolerability, up to a maximum maintenance dose of 15 mg once weekly.
The extended half-life also means that if a dose is missed, there is some flexibility in administration. According to the MHRA/EMC SmPC, if a dose is missed, it should be administered as soon as possible within 4 days (96 hours) of the missed dose. If more than 4 days have passed, the missed dose should be skipped, and the next dose should be taken on the regularly scheduled day. Additionally, patients can change their weekly injection day if necessary, provided there are at least 3 days (72 hours) between doses.
Patients should be advised to maintain consistency with their dosing schedule whenever possible. The long half-life means that it takes approximately 4 to 5 weeks to reach steady-state concentrations, and similarly, it takes several weeks for the drug to be fully eliminated from the body after discontinuation. This has implications for dose adjustments—changes in dose will not produce immediate effects, and clinicians should allow adequate time (typically 4 weeks) to assess the full impact of a dose increase before making further adjustments. When Mounjaro is used with sulfonylureas or insulin, the dose of these medications may need to be reduced to minimise the risk of hypoglycaemia. Patients should be counselled about realistic expectations regarding the timeline for therapeutic effects and the importance of recognising and managing hypoglycaemia if it occurs.
When treatment with Mounjaro is discontinued, the medication does not leave the body immediately due to its extended half-life. It takes approximately 5 half-lives for a drug to be considered essentially eliminated from the system, which means tirzepatide may remain detectable in the body for approximately 25 days (around 3 to 4 weeks) after the last injection. During this washout period, the drug continues to exert some metabolic effects, though these gradually diminish as concentrations decline.
Patients who stop taking Mounjaro may experience a gradual return of previous symptoms associated with type 2 diabetes, including elevated blood glucose levels and potential weight regain. The rate and extent of these changes vary considerably between individuals and depend on factors such as baseline disease severity, concurrent medications, lifestyle factors, and the duration of prior Mounjaro treatment. Some patients may notice changes within a few weeks, whilst others may experience a more gradual transition. No specific withdrawal syndrome has been reported in clinical trials, but the loss of glycaemic control and appetite suppression can be clinically significant.
Patients should never stop taking Mounjaro without consulting their GP or diabetes specialist. Abrupt discontinuation without appropriate alternative management may lead to deterioration in glycaemic control, which can increase the risk of diabetes-related complications. If discontinuation is necessary—due to side effects, pregnancy planning, or other medical reasons—healthcare professionals will typically arrange for alternative diabetes management strategies, which may include other medications, intensified lifestyle interventions, or closer monitoring.
Mounjaro is not recommended during pregnancy, and women of childbearing potential should use effective contraception while taking tirzepatide. Women planning pregnancy should discontinue tirzepatide in advance, as advised by their healthcare provider. Patients should be aware that tirzepatide can reduce the effectiveness of oral contraceptives, particularly during initiation and dose increases, and should use additional or alternative contraceptive methods for 4 weeks after starting treatment and for 4 weeks after each dose increase.
Patients should seek urgent medical attention if they experience severe, persistent abdominal pain (which may radiate to the back, with or without vomiting) as this could indicate pancreatitis, or if they develop symptoms of gallbladder disease, or persistent vomiting and diarrhoea leading to dehydration.
Whilst the half-life of Mounjaro is relatively consistent across most patients, several patient-specific factors may theoretically influence how the drug is processed and eliminated from the body. Understanding these factors helps clinicians personalise treatment and anticipate potential variations in drug response.
Renal function is one consideration, as the kidneys play a role in eliminating many medications. According to the MHRA/EMC SmPC, no dose adjustment of tirzepatide is required in patients with renal impairment, including those with end-stage renal disease (ESRD). However, patients with kidney disease should have their renal function monitored regularly as part of routine diabetes care, especially if they experience significant gastrointestinal adverse effects that could lead to dehydration and acute kidney injury.
Hepatic function may also theoretically affect drug metabolism, though tirzepatide is primarily eliminated through protein degradation rather than hepatic metabolism. Clinical data suggest that mild to moderate hepatic impairment does not significantly alter tirzepatide exposure, and no dose adjustment is recommended. There is limited clinical experience in patients with severe hepatic impairment.
Body weight and composition may influence the volume of distribution and drug concentrations, though the clinical significance appears limited. Age, sex, and ethnicity have been evaluated in clinical trials, and no clinically meaningful differences in pharmacokinetics have been identified that would necessitate dose adjustments. Drug interactions affecting tirzepatide's half-life are uncommon, as it is not metabolised by cytochrome P450 enzymes. However, because Mounjaro delays gastric emptying, it may affect the absorption of oral medications, particularly those requiring rapid absorption or with narrow therapeutic windows.
A notable interaction involves oral contraceptives. The SmPC advises that women using oral contraceptives should take additional precautions for 4 weeks after starting tirzepatide and for 4 weeks after each dose increase, or consider using a non-oral contraceptive method. Patients taking other time-sensitive medications should discuss timing strategies with their healthcare provider to ensure optimal efficacy of all treatments. Patients with pre-existing diabetic retinopathy should also be monitored for progression of retinopathy, particularly during periods of rapid improvement in glycaemic control.
Mounjaro (tirzepatide) may remain detectable in the body for approximately 25 days (3–4 weeks) after the last injection, as it takes about 5 half-lives for the drug to be essentially eliminated. During this period, metabolic effects gradually diminish as drug concentrations decline.
Yes, you can change your weekly Mounjaro injection day provided there are at least 3 days (72 hours) between doses. Maintaining consistency with your dosing schedule is recommended whenever possible.
No dose adjustment of Mounjaro is required for renal impairment or mild-to-moderate hepatic impairment, as tirzepatide is primarily eliminated through protein degradation rather than renal or hepatic pathways. However, regular monitoring of kidney function is advised as part of routine diabetes care.
All medical content on this blog is created based on reputable, evidence-based sources and reviewed regularly for accuracy and relevance. While we strive to keep content up to date with the latest research and clinical guidelines, it is intended for general informational purposes only.
DisclaimerThis content is not a substitute for professional medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional with any medical questions or concerns. Use of the information is at your own risk, and we are not responsible for any consequences resulting from its use.