
Many patients in the UK require treatment for both type 2 diabetes and mental health conditions such as depression or anxiety. Mounjaro (tirzepatide), a once-weekly injection for type 2 diabetes, and sertraline, a commonly prescribed antidepressant, are frequently used together. Understanding whether does Mounjaro interact with sertraline is essential for safe medication management. Fortunately, no direct pharmacological interaction exists between these two medications, and they can generally be taken concurrently. However, patients should be aware of important safety considerations, particularly regarding gastrointestinal side effects and monitoring requirements, to ensure optimal treatment outcomes.
Quick Answer: Mounjaro (tirzepatide) does not have a direct pharmacological interaction with sertraline, and the two medications can generally be taken together safely without dose adjustments.

Mounjaro® is the most innovative GLP-1 medication proven to dramatically curb appetite, hunger, and cravings to help professional men achieve substantial weight loss.
Start Here
Wegovy® is a weekly injectable GLP-1 medication with proven effectiveness in reducing appetite, hunger, and cravings to help busy professionals lose significant weight.
Start HereMounjaro (tirzepatide) and sertraline are two distinct medications prescribed for entirely different medical conditions, yet patients may find themselves taking both concurrently due to the prevalence of their respective indications.
Mounjaro is a glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like peptide-1 (GLP-1) receptor agonist licensed in the UK specifically for the treatment of type 2 diabetes mellitus. Administered as a once-weekly subcutaneous injection, Mounjaro helps improve glycaemic control by enhancing insulin secretion, suppressing glucagon release, and slowing gastric emptying. The medication received marketing authorisation for use in the UK for type 2 diabetes management. According to NICE guidance (TA849), tirzepatide may be considered as an option for treating insufficiently controlled type 2 diabetes in adults, typically as an add-on therapy when metformin or other oral agents are insufficient. While using Mounjaro, many patients experience weight reduction, which can be beneficial for those with type 2 diabetes and obesity, though this is not its primary licensed indication in the UK.
Sertraline, by contrast, is a selective serotonin reuptake inhibitor (SSRI) antidepressant widely prescribed for depression, anxiety disorders, obsessive-compulsive disorder (OCD), post-traumatic stress disorder (PTSD), and panic disorder. It works by increasing serotonin levels in the brain, thereby improving mood and emotional regulation. Sertraline has been available in the UK for decades and is commonly prescribed for mental health conditions due to its established efficacy and generally favourable side-effect profile compared to some alternatives.
Given that type 2 diabetes and depression frequently co-exist—with studies suggesting that individuals with diabetes are approximately twice as likely to experience depression—it is not uncommon for patients to require treatment with both Mounjaro and sertraline simultaneously.
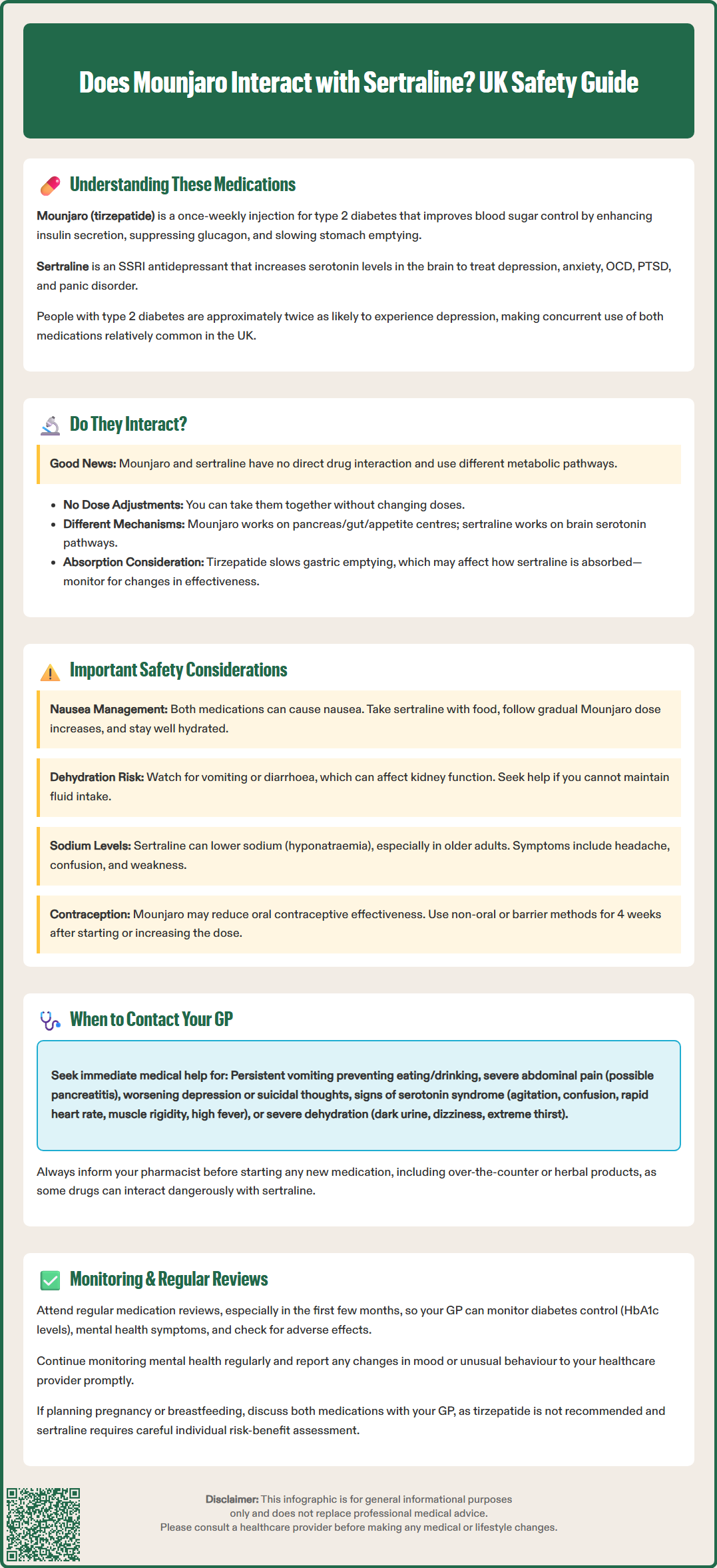
The reassuring news for patients and clinicians alike is that no direct pharmacokinetic or pharmacodynamic interaction between Mounjaro (tirzepatide) and sertraline is listed in their respective Summary of Product Characteristics (SmPCs) or the British National Formulary (BNF).
Mounjaro is a peptide-based medication that is metabolised primarily through proteolytic degradation rather than hepatic cytochrome P450 enzyme pathways. Sertraline is metabolised extensively in the liver (predominantly via CYP2C19, CYP2B6, CYP3A4, and CYP2D6 enzymes), and is a mild inhibitor of CYP2D6. However, this does not affect tirzepatide metabolism, as the medications do not share significant metabolic pathways that would lead to clinically relevant interactions.
No dose adjustments are routinely recommended when initiating or continuing either medication in the presence of the other. The SmPC for Mounjaro does not list sertraline as a contraindication or as requiring special precautions, and similarly, sertraline's prescribing information does not flag concerns regarding concurrent GLP-1 receptor agonist use.
However, there are important considerations:
Tirzepatide slows gastric emptying, which can potentially affect the absorption of orally administered medications, including sertraline. Patients should be monitored for changes in clinical response to sertraline after starting or increasing the dose of tirzepatide.
Oral contraceptive exposure may be reduced when starting or increasing tirzepatide doses. The Mounjaro SmPC advises using non-oral contraception or adding a barrier method for 4 weeks after initiation and after each dose increase.
Hyponatraemia risk with SSRIs like sertraline should be considered, particularly in older adults or those taking diuretics. This risk could potentially be compounded if dehydration occurs due to gastrointestinal side effects from tirzepatide.
Both medications can cause gastrointestinal side effects independently—Mounjaro commonly causes nausea, vomiting, and diarrhoea, whilst sertraline may also produce nausea and gastrointestinal upset, particularly during the initial weeks of treatment. When taken together, these effects might be additive, potentially affecting patient tolerability and adherence.
Understanding the distinct mechanisms of action of Mounjaro and sertraline helps clarify why they do not have a direct pharmacological interaction.
Mounjaro's mechanism of action involves dual agonism at both GIP and GLP-1 receptors, as described in its SmPC. These are incretin hormones naturally released by the gut in response to food intake. By activating these receptors, tirzepatide:
Enhances glucose-dependent insulin secretion from pancreatic beta cells, helping to lower blood glucose levels when they are elevated
Suppresses inappropriate glucagon release from pancreatic alpha cells, reducing hepatic glucose production
Slows gastric emptying, which moderates the rate at which glucose enters the bloodstream after meals
Promotes satiety through central nervous system pathways, contributing to reduced caloric intake and weight loss
These actions occur primarily at the level of the pancreas, gastrointestinal tract, and specific brain regions involved in appetite regulation. Mounjaro does not significantly affect neurotransmitter systems such as serotonin, dopamine, or noradrenaline.
Sertraline's mechanism of action is entirely different. As an SSRI, sertraline selectively inhibits the reuptake of serotonin (5-hydroxytryptamine, or 5-HT) at the presynaptic neuronal membrane in the central nervous system. This inhibition increases the availability of serotonin in the synaptic cleft, enhancing serotonergic neurotransmission. Over time, this leads to:
Improved mood and reduced symptoms of depression
Decreased anxiety and intrusive thoughts
Better emotional regulation
Sertraline's effects are confined primarily to the central nervous system. While sertraline does not directly influence glucose metabolism or incretin hormone activity, it's worth noting that SSRIs may alter glycaemic control in some individuals. Therefore, regular monitoring of blood glucose and HbA1c is advisable when starting or changing sertraline dosage in people with diabetes. The lack of substantial overlap in their primary sites and mechanisms of action explains why these medications can generally be co-administered without direct pharmacological interference.
Whilst Mounjaro and sertraline do not interact directly, several practical safety considerations should be kept in mind when taking both medications concurrently.
Gastrointestinal tolerability is perhaps the most relevant consideration. Both medications can independently cause nausea, particularly during treatment initiation. Mounjaro's nausea typically occurs due to delayed gastric emptying and is most pronounced during dose escalation. Sertraline-related nausea usually improves after the first few weeks of treatment. When starting both medications together, or adding one to an established regimen of the other, patients should:
Take sertraline with food to minimise gastric irritation
Follow the gradual dose titration schedule for Mounjaro as prescribed
Stay well hydrated, especially if experiencing vomiting or diarrhoea
Report persistent or severe gastrointestinal symptoms to their GP
Risk of dehydration and kidney function: If significant vomiting or diarrhoea occurs, it's important to maintain adequate hydration. In some cases, particularly in those with pre-existing kidney disease, renal function monitoring may be necessary. Seek medical advice if unable to maintain fluid intake or experiencing signs of dehydration.
Hypoglycaemia awareness is another important consideration. Whilst Mounjaro has a low intrinsic risk of hypoglycaemia when used alone, patients taking it alongside other glucose-lowering medications (such as sulphonylureas or insulin) may be at increased risk. Depression and anxiety can sometimes affect a patient's ability to recognise or respond appropriately to hypoglycaemic symptoms. Patients should be educated about recognising signs of low blood glucose (tremor, sweating, confusion, palpitations) and the importance of regular blood glucose monitoring.
Hyponatraemia risk: SSRIs like sertraline can cause hyponatraemia (low sodium levels), particularly in older adults or those taking diuretics. This risk could potentially be compounded if dehydration occurs due to tirzepatide's gastrointestinal effects. Symptoms include headache, confusion, weakness, and in severe cases, seizures.
Bleeding risk: Sertraline may increase the risk of bleeding, particularly when combined with medications like aspirin, NSAIDs (e.g., ibuprofen), or anticoagulants (e.g., warfarin, direct oral anticoagulants). Discuss all medications with your healthcare provider.
Contraception considerations: Tirzepatide may reduce the effectiveness of oral contraceptives. The SmPC advises using non-oral contraception or adding a barrier method for 4 weeks after starting tirzepatide and after each dose increase.
Mental health monitoring remains essential. Type 2 diabetes itself can impact mood and quality of life, and patients should continue regular follow-up with their GP or mental health team to assess the effectiveness of sertraline. Any worsening of depressive symptoms, emergence of suicidal thoughts, or unusual behavioural changes should be reported immediately.
Medication adherence can be supported by establishing a consistent routine. Taking sertraline at the same time each day (many patients prefer morning dosing to minimise potential sleep disturbance) and administering Mounjaro on the same day each week helps maintain therapeutic levels and optimise treatment outcomes.
Whilst Mounjaro and sertraline can generally be taken together safely, certain situations warrant prompt discussion with your healthcare team.
Contact your GP or pharmacist if you experience:
Severe or persistent nausea and vomiting that prevents you from eating, drinking, or taking your medications
Signs of dehydration, including dark urine, dizziness, reduced urination, or extreme thirst
Unexplained abdominal pain, particularly if severe or accompanied by vomiting—this could indicate pancreatitis, a rare but serious side effect of GLP-1 receptor agonists. If pancreatitis is suspected, stop taking tirzepatide and seek urgent medical advice
Symptoms of hypoglycaemia that are frequent, severe, or difficult to manage
Worsening depression, anxiety, or suicidal thoughts—this requires urgent medical attention
Unusual bleeding or bruising, as sertraline can affect platelet function
Symptoms of hyponatraemia such as headache, confusion, weakness, or seizures
Symptoms of serotonin syndrome such as agitation, confusion, rapid heart rate, high blood pressure, dilated pupils, muscle rigidity, or high fever. This is rare but can occur with sertraline, particularly when combined with other serotonergic medications (e.g., other antidepressants, tramadol, triptans, St John's wort, or certain illicit drugs)
In an emergency:
Call 999 if you experience severe chest or abdominal pain, signs of a severe allergic reaction, severe confusion, high fever, or seizures
Contact NHS 111 for urgent but non-emergency advice when your GP is unavailable
Before starting any new medication (prescription, over-the-counter, or herbal), inform your pharmacist that you are taking both Mounjaro and sertraline. Some medications may interact with one or both of these drugs. For example, non-steroidal anti-inflammatory drugs (NSAIDs) can increase bleeding risk when taken with sertraline.
Regular medication reviews are important, particularly in the first few months of treatment. Your GP should monitor your HbA1c levels to assess diabetes control (as recommended in NICE guideline NG28), review your mental health symptoms to evaluate sertraline's effectiveness, and check for any adverse effects.
If you are planning pregnancy or are breastfeeding, discuss both medications with your GP. Tirzepatide is not recommended during pregnancy or breastfeeding according to its SmPC. Sertraline use in pregnancy requires careful individual risk-benefit assessment, though it is often considered one of the preferred SSRIs when antidepressant treatment is necessary during pregnancy or breastfeeding.
If you experience any side effects from either medication, you can report them through the MHRA Yellow Card Scheme, which helps monitor the safety of medicines in the UK.
Yes, Mounjaro (tirzepatide) and sertraline can be taken together safely, as there is no direct pharmacological interaction between them. No dose adjustments are routinely required, though patients should be monitored for gastrointestinal side effects and changes in clinical response.
Mounjaro slows gastric emptying, which could theoretically affect the absorption of oral medications like sertraline. However, clinically significant effects are uncommon, and patients should be monitored for any changes in mental health symptoms after starting or adjusting tirzepatide doses.
Both medications can cause nausea and gastrointestinal upset, which may be more pronounced when taken together. Watch for severe or persistent nausea, vomiting, dehydration, signs of low blood sugar, worsening depression, or symptoms of hyponatraemia, and contact your GP if these occur.
All medical content on this blog is created based on reputable, evidence-based sources and reviewed regularly for accuracy and relevance. While we strive to keep content up to date with the latest research and clinical guidelines, it is intended for general informational purposes only.
DisclaimerThis content is not a substitute for professional medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional with any medical questions or concerns. Use of the information is at your own risk, and we are not responsible for any consequences resulting from its use.