
GLP-1 receptor agonists, such as semaglutide and liraglutide, are widely prescribed in the UK for type 2 diabetes and weight management. Whilst these medications offer significant therapeutic benefits, gastrointestinal side effects—including bloating—are commonly reported. Understanding whether GLP-1 medications help or hinder bloating is essential for patients and prescribers alike. This article examines the relationship between GLP-1 therapy and bloating, explores the underlying mechanisms, and provides evidence-based guidance on managing symptoms. We also outline when medical review is necessary to ensure safe and effective treatment.
Quick Answer: GLP-1 receptor agonists do not treat bloating; rather, they may cause or worsen bloating as a gastrointestinal side effect due to delayed gastric emptying.

Mounjaro® is the most innovative GLP-1 medication proven to dramatically curb appetite, hunger, and cravings to help professional men achieve substantial weight loss.
Start Here
Wegovy® is a weekly injectable GLP-1 medication with proven effectiveness in reducing appetite, hunger, and cravings to help busy professionals lose significant weight.
Start HereGlucagon-like peptide-1 (GLP-1) receptor agonists are a class of medications with specific licensed indications in the UK. They are primarily prescribed for the management of type 2 diabetes mellitus (semaglutide [Ozempic], liraglutide [Victoza], dulaglutide [Trulicity], exenatide [Byetta, Bydureon BCise]) and, with separate formulations, for weight management in adults with obesity or overweight with weight-related comorbidities (semaglutide [Wegovy], liraglutide [Saxenda]).
These medications work by mimicking the action of naturally occurring GLP-1, a hormone released by the intestine in response to food intake. GLP-1 receptor agonists bind to GLP-1 receptors throughout the body, triggering several physiological responses that help regulate blood glucose levels. The primary mechanisms include:
Enhancing insulin secretion from pancreatic beta cells in a glucose-dependent manner, which means insulin is released only when blood glucose levels are elevated
Suppressing glucagon release from pancreatic alpha cells, thereby reducing hepatic glucose production
Slowing gastric emptying, which delays the rate at which food leaves the stomach and enters the small intestine
Reducing appetite through central nervous system effects, promoting satiety and decreasing food intake
The slowing of gastric emptying is particularly relevant when considering gastrointestinal side effects. By prolonging the time food remains in the stomach, GLP-1 medications can affect digestive processes and may contribute to various gastrointestinal symptoms. This mechanism, whilst beneficial for glucose control and weight management, can lead to feelings of fullness, nausea, and potentially bloating in some individuals.
It's important to note that GLP-1 receptor agonists are generally not recommended for people with severe gastrointestinal disease or gastroparesis, as stated in their Summary of Product Characteristics (SmPCs).
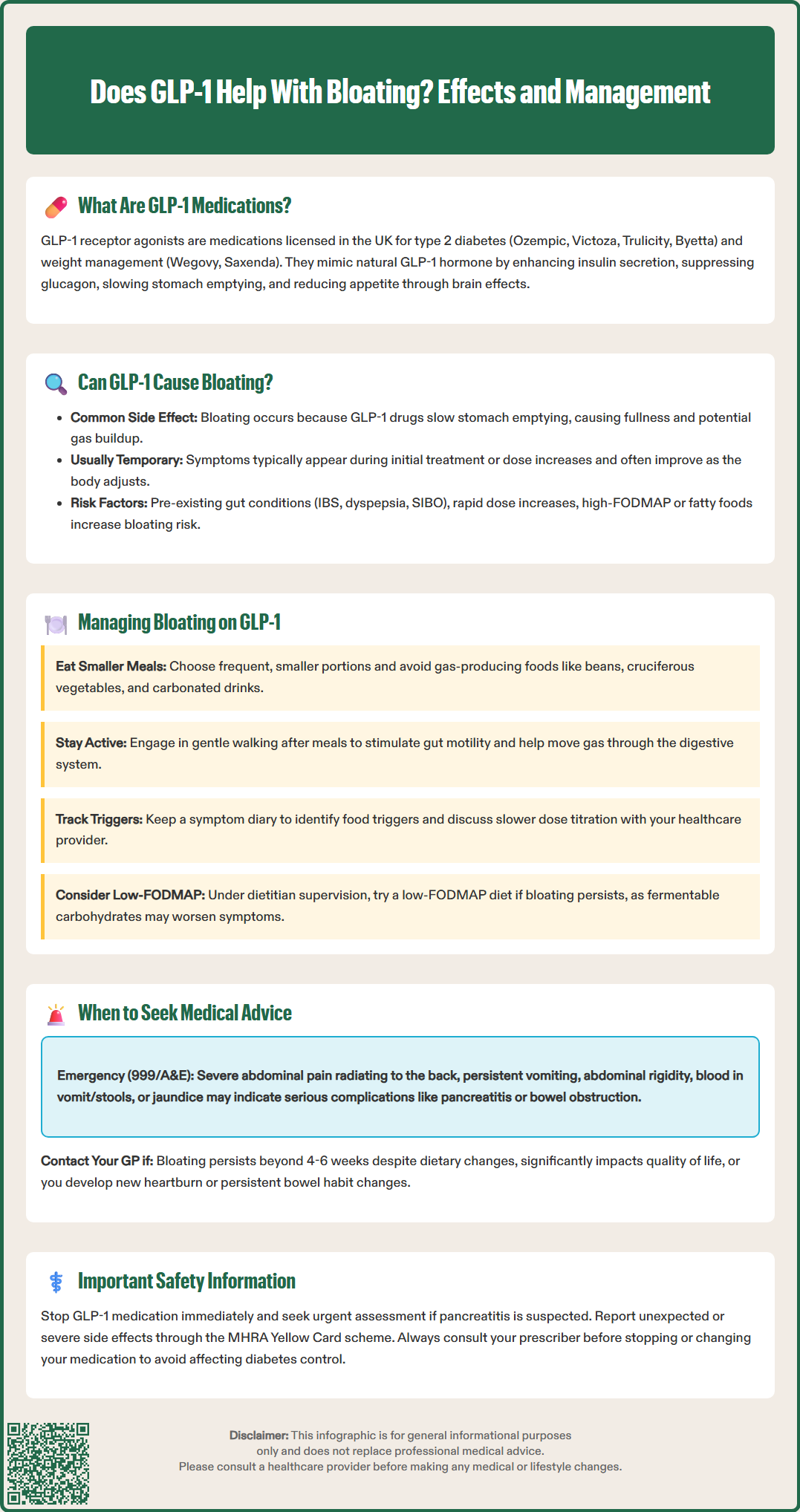
Gastrointestinal symptoms are common side effects associated with GLP-1 receptor agonist therapy. According to the SmPCs for these medications, the most frequently reported gastrointestinal adverse effects include nausea, vomiting, diarrhoea, constipation, abdominal pain, abdominal distension, dyspepsia and flatulence. While bloating (often described as abdominal distension in clinical terms) is reported by patients, it is generally less commonly reported than nausea or diarrhoea. Clinical trial data and post-marketing surveillance indicate that gastrointestinal adverse effects are among the most frequent reasons for treatment discontinuation.
The mechanism by which GLP-1 medications may contribute to bloating relates primarily to delayed gastric emptying. When the stomach empties more slowly, this can lead to:
A sensation of abdominal fullness or distension
Altered bowel motility patterns affecting the transit of intestinal contents
Potential changes in digestive processes
Possible gas accumulation in the digestive tract
It is important to note that there is no official indication for GLP-1 medications as a treatment for bloating; rather, bloating may occur as an adverse effect in susceptible individuals. The severity and duration of gastrointestinal symptoms vary considerably between patients. Many individuals experience transient gastrointestinal symptoms during the initial weeks of treatment or following dose escalation, with symptoms often improving as the body adapts to the medication.
Certain factors may increase the likelihood of experiencing bloating on GLP-1 therapy, including:
Pre-existing gastrointestinal conditions such as irritable bowel syndrome (IBS), functional dyspepsia, or small intestinal bacterial overgrowth (SIBO)
Rapid dose escalation without adequate titration periods
Dietary factors, particularly high intake of fermentable carbohydrates (FODMAPs), fatty foods, or carbonated beverages
Concurrent medications that affect gastrointestinal motility
Patients should be aware that GLP-1 receptor agonists have been associated with more serious gastrointestinal adverse effects, including pancreatitis (inflammation of the pancreas) and gallbladder disease. Recent pharmacovigilance has also identified signals for intestinal obstruction (ileus) with some GLP-1 receptor agonists. These conditions can present with abdominal symptoms and require prompt medical attention.
For patients experiencing bloating whilst taking GLP-1 receptor agonists, several evidence-based strategies may help alleviate symptoms without necessarily requiring treatment discontinuation. NICE guidance on diabetes management (NG28) emphasises the importance of supporting patients through adverse effects to optimise treatment adherence and outcomes.
Dietary modifications often provide the first line of symptom management:
Eat smaller, more frequent meals rather than large portions, which can overwhelm the already-slowed digestive system
Reduce intake of gas-producing foods such as beans, lentils, cruciferous vegetables (broccoli, cauliflower, cabbage), onions, and carbonated drinks
Limit high-fat foods, as these delay gastric emptying further and may compound the medication's effects
Consider a low-FODMAP approach under dietitian supervision if symptoms are persistent, as fermentable carbohydrates can contribute to bloating
Stay well-hydrated with still water throughout the day to support digestive function
Avoid eating close to bedtime, allowing at least 3 hours between the last meal and lying down
Lifestyle adjustments can also prove beneficial:
Regular physical activity, particularly gentle walking after meals, can stimulate gastrointestinal motility and help move gas through the digestive tract
Stress management techniques such as mindfulness or breathing exercises, as stress can exacerbate gastrointestinal symptoms
Maintaining a symptom diary to identify specific food triggers or patterns
Medication-related strategies should be discussed with your prescribing healthcare professional:
Slower dose titration may reduce the intensity of gastrointestinal side effects
Pausing escalation or stepping back to a previously tolerated dose if symptoms are troublesome
Timing of administration considerations (note that while most GLP-1 RAs are not meal-timed, exenatide immediate-release [Byetta] is taken before meals)
Review of concurrent medications that may contribute to bloating, such as certain antibiotics, opioids, or iron supplements
Over-the-counter remedies such as simeticone (an anti-foaming agent) or peppermint oil capsules may provide symptomatic relief for some individuals, though evidence for their effectiveness varies. Note that peppermint oil may worsen symptoms in those with gastro-oesophageal reflux disease (GORD). Probiotic supplements have been studied for various gastrointestinal complaints, but there is insufficient evidence to recommend specific strains for GLP-1-related bloating. Always consult your GP or pharmacist before starting any new supplements, as interactions may occur.
Whilst mild bloating is relatively common during GLP-1 therapy and often resolves with time and dietary adjustments, certain symptoms warrant prompt medical evaluation. Patients should be advised to contact their GP or NHS 111 if they experience:
Red flag symptoms requiring urgent assessment:
Severe, persistent abdominal pain, particularly if in the upper abdomen and radiating to the back (may indicate pancreatitis)
Severe abdominal pain and distension with vomiting and inability to pass wind or stools (may indicate bowel obstruction)
Persistent vomiting, particularly if unable to keep down fluids, raising concerns about dehydration
Abdominal distension with rigidity or extreme tenderness on palpation
Blood in vomit or stools (melaena or haematochezia)
Unintentional weight loss beyond expected therapeutic effects
Fever accompanying abdominal symptoms, which may suggest infection or inflammation
Right upper quadrant pain or jaundice (yellowing of skin/eyes), which may indicate gallbladder disease
For severe symptoms, call 999 or go to A&E immediately.
Symptoms requiring routine medical review:
Bloating that persists beyond 4–6 weeks despite dietary modifications and adequate dose titration
Symptoms that significantly impact quality of life or ability to maintain adequate nutrition
New or worsening heartburn or regurgitation, which may indicate gastro-oesophageal reflux disease (GORD)
Changes in bowel habit such as persistent diarrhoea or constipation
Concerns about medication adherence due to gastrointestinal side effects
Your healthcare professional may recommend investigations to exclude other causes of bloating, particularly if symptoms are atypical or severe. These might include:
Blood tests to assess for coeliac disease, inflammatory markers, or thyroid function
Breath tests for lactose intolerance or small intestinal bacterial overgrowth
Abdominal imaging (ultrasound or CT) if structural abnormalities are suspected
Faecal calprotectin if inflammatory bowel disease is a concern
Referral to gastroenterology for specialist assessment if symptoms persist despite initial management
The MHRA's Yellow Card scheme allows patients and healthcare professionals to report suspected side effects of medications, including GLP-1 agonists. If you experience unexpected or severe symptoms, reporting through this system contributes to ongoing medication safety monitoring.
Important: If pancreatitis is suspected (severe persistent abdominal pain, with or without vomiting), you should stop taking the GLP-1 medication and seek urgent medical assessment, as advised in the product information. For other gastrointestinal symptoms, consult your prescriber before making any changes to your treatment regimen, as this may affect glycaemic control in diabetes management.
Yes, GLP-1 receptor agonists can cause bloating as a side effect due to delayed gastric emptying, which slows digestion and may lead to abdominal distension. Symptoms often improve with time and dietary adjustments.
Eating smaller, more frequent meals, avoiding gas-producing and high-fat foods, staying hydrated, and engaging in gentle physical activity after meals can help alleviate bloating. Discuss slower dose titration with your prescriber if symptoms persist.
Seek urgent medical attention if you experience severe abdominal pain, persistent vomiting, inability to pass wind or stools, blood in vomit or stools, or jaundice. Routine review is advised if bloating persists beyond 4–6 weeks or significantly impacts quality of life.
All medical content on this blog is created based on reputable, evidence-based sources and reviewed regularly for accuracy and relevance. While we strive to keep content up to date with the latest research and clinical guidelines, it is intended for general informational purposes only.
DisclaimerThis content is not a substitute for professional medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional with any medical questions or concerns. Use of the information is at your own risk, and we are not responsible for any consequences resulting from its use.