
Saxenda (liraglutide 3.0 mg) is a GLP-1 receptor agonist licensed for weight management in the UK. Many patients wonder whether they can stay on the same dose of Saxenda long-term once they reach the maintenance level. The standard treatment protocol involves gradual dose escalation over five weeks to reach 3.0 mg daily, which is designed for ongoing use. Understanding dosing requirements, when adjustments may be necessary, and how to maintain treatment safely helps ensure optimal outcomes. This article examines the evidence and guidance around maintaining a stable Saxenda dose throughout your treatment journey.
Quick Answer: Yes, once you reach the maintenance dose of 3.0 mg daily, you are expected to remain on this dose throughout treatment, provided it is well tolerated and effective.

Mounjaro® is the most innovative GLP-1 medication proven to dramatically curb appetite, hunger, and cravings to help professional men achieve substantial weight loss.
Start Here
Wegovy® is a weekly injectable GLP-1 medication with proven effectiveness in reducing appetite, hunger, and cravings to help busy professionals lose significant weight.
Start HereSaxenda (liraglutide 3.0 mg) is a glucagon-like peptide-1 (GLP-1) receptor agonist licensed in the UK for weight management in adults with a body mass index (BMI) of 30 kg/m² or greater, or 27 kg/m² or greater in the presence of weight-related comorbidities. The medication works by mimicking the action of the naturally occurring hormone GLP-1, which regulates appetite and food intake by acting on receptors in the brain that control hunger signals.
The standard dosing protocol for Saxenda involves a gradual titration schedule designed to minimise gastrointestinal side effects whilst allowing the body to adjust to the medication. Treatment begins with a starting dose of 0.6 mg administered once daily via subcutaneous injection. This dose is then increased weekly in 0.6 mg increments: 1.2 mg in week two, 1.8 mg in week three, 2.4 mg in week four, and finally reaching the maintenance dose of 3.0 mg daily from week five onwards.
This titration approach is specified in the UK Summary of Product Characteristics (SmPC). The gradual increase helps reduce the likelihood and severity of common adverse effects such as nausea, vomiting, diarrhoea, and constipation, which are most pronounced when treatment is initiated or doses are increased too rapidly.
Key points about Saxenda titration:
The standard maintenance dose is 3.0 mg once daily
Titration typically occurs over five weeks
Slower titration may be considered if gastrointestinal symptoms are problematic
The medication can be administered once daily at any time of day, with or without food; choosing a consistent time aids adherence
If you miss a dose: If a dose is missed and the next scheduled dose is due within 12 hours, skip the missed dose. Do not take an extra dose or increase the next dose to make up for the missed one. If more than 3 days have passed since your last dose, restart at 0.6 mg and follow the titration schedule again to reduce gastrointestinal side effects.
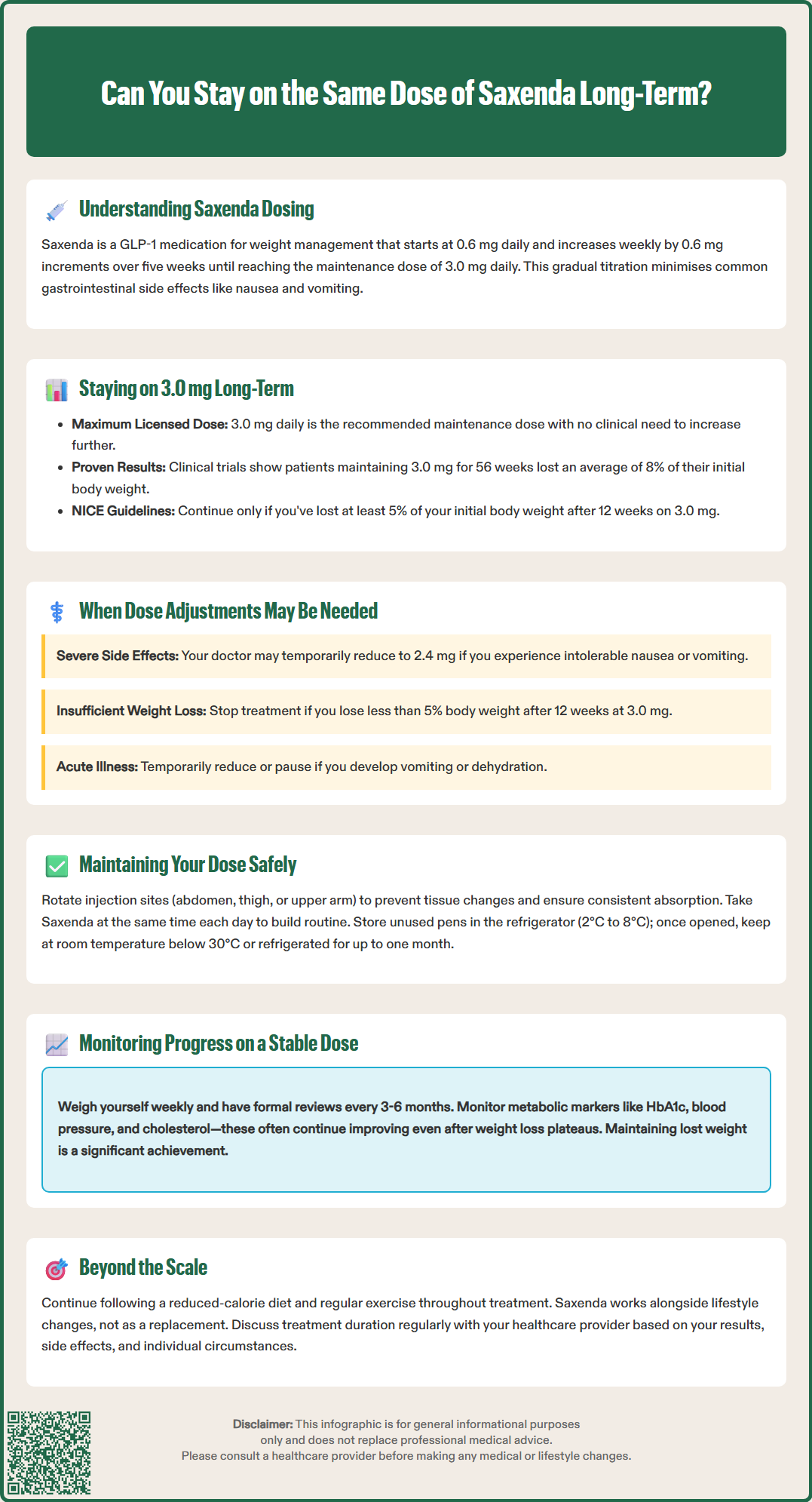
Once you have reached the maintenance dose of 3.0 mg daily, it is both appropriate and expected that you will remain on this dose for the duration of your treatment, provided it is well tolerated and effective. There is no clinical requirement to continue increasing the dose beyond 3.0 mg, as this represents the maximum licensed dose for weight management in the UK.
Clinical trial evidence supporting Saxenda's efficacy, including the SCALE (Satiety and Clinical Adiposity – Liraglutide Evidence) programme, demonstrates that patients who maintain the 3.0 mg daily dose achieve significant and sustained weight loss over extended periods. The pivotal SCALE Obesity and Prediabetes trial showed that participants maintaining this dose for 56 weeks achieved an average weight loss of 8% of their initial body weight, compared to 2.6% in the placebo group.
For some individuals who experience intolerable side effects at the 3.0 mg dose, remaining on a lower maintenance dose (such as 2.4 mg or 1.8 mg) may be considered after discussion with their prescribing clinician. This would be an off-label use requiring individualised clinical judgement and documentation. Whilst the 3.0 mg dose provides optimal efficacy, a lower dose that is well tolerated and produces meaningful weight loss may be preferable to discontinuing treatment altogether in some cases.
Important considerations:
The 3.0 mg dose is designed for long-term maintenance
Continuing on the same effective dose is the standard approach
Lower maintenance doses represent off-label use requiring clinical judgement
Treatment duration should be reviewed regularly with your healthcare provider
NICE Technology Appraisal 664 (TA664) recommends that Saxenda should only be continued beyond 12 weeks if patients have lost at least 5% of their initial body weight after 12 weeks on the 3.0 mg dose, emphasising the importance of demonstrable efficacy at the prescribed dose.
Whilst most patients remain on the 3.0 mg maintenance dose throughout their treatment, certain clinical situations may necessitate dose adjustments. Understanding when and why modifications might be required helps ensure safe and effective use of Saxenda.
Tolerability issues represent the most common reason for dose adjustment. If you experience persistent or severe gastrointestinal symptoms (nausea, vomiting, diarrhoea) at the 3.0 mg dose that significantly impact your quality of life, your prescriber may recommend temporarily reducing to the previous dose level (2.4 mg) for one additional week before attempting to increase again. If symptoms remain intolerable despite this approach, maintaining treatment at a lower dose may be discussed, though this would be off-label use.
Inadequate weight loss response may prompt clinical review. NICE TA664 stipulates that treatment should be discontinued if less than 5% weight loss is achieved after 12 weeks at the 3.0 mg maintenance dose. In such cases, continuing at the same dose is unlikely to produce meaningful benefit, and alternative weight management strategies should be explored rather than dose escalation beyond the licensed maximum.
Concurrent illness or medication changes may also influence dosing decisions. If you develop acute illness causing vomiting or dehydration, temporary dose reduction or treatment interruption may be necessary. For patients taking warfarin or other coumarin anticoagulants, increased INR monitoring may be required when starting Saxenda. For patients with type 2 diabetes, dose adjustments to diabetes medications (particularly sulfonylureas or insulin) may be required to reduce hypoglycaemia risk, though the Saxenda dose itself typically remains unchanged.
Pregnancy and breastfeeding require immediate discontinuation of Saxenda, as safety data in these populations are insufficient. If you are planning pregnancy or discover you are pregnant, contact your healthcare provider immediately to discuss stopping treatment.
Renal or hepatic impairment: No dose adjustment is recommended for patients with mild to moderate renal or hepatic impairment. However, Saxenda is not recommended for use in patients with severe hepatic impairment or end-stage renal disease due to limited clinical data in these populations.
Remaining on a stable Saxenda dose requires attention to several practical and clinical considerations to optimise safety and effectiveness. Consistent administration technique and timing contribute significantly to treatment success and tolerability.
Injection technique and site rotation are fundamental to safe long-term use. Saxenda should be injected subcutaneously into the abdomen, thigh, or upper arm. Rotating injection sites within these areas helps prevent lipodystrophy (changes in fat tissue) and ensures consistent absorption. Avoid injecting into the same spot repeatedly, and inspect injection sites regularly for signs of irritation, lumps, or skin changes. If you notice persistent problems at injection sites, discuss this with your prescriber or practice nurse.
Timing consistency enhances treatment adherence. Saxenda can be administered at any time of day, independent of meals. Choosing a consistent time daily helps establish a routine that supports adherence. The medication can be taken with or without food according to personal preference.
Storage and handling require careful attention. Saxenda pens should be stored in a refrigerator (2°C to 8°C) before first use. Once in use, the pen may be stored at room temperature (below 30°C) or in the refrigerator for up to one month. Never freeze Saxenda, and discard any pens that have been frozen. Keep the pen cap on when not in use to protect from light.
Managing persistent side effects whilst maintaining your dose involves several strategies:
Eat smaller, more frequent meals rather than large portions
Avoid high-fat, greasy, or spicy foods that may exacerbate nausea
Stay well hydrated, particularly if experiencing diarrhoea
Consider taking the injection at bedtime if daytime nausea is problematic
When to seek medical advice:
Severe or persistent abdominal pain (potential pancreatitis) – stop Saxenda and seek urgent medical attention
Signs of dehydration (dizziness, reduced urination, extreme thirst)
Symptoms of gallbladder disease (pain in upper right abdomen, yellowing of skin or eyes)
Unexplained rapid heartbeat or palpitations
Signs of allergic reaction (rash, swelling, difficulty breathing)
If you experience side effects, report them through the MHRA Yellow Card scheme (yellowcard.mhra.gov.uk) to help monitor the safety of this medication.
Regular monitoring whilst maintaining a stable Saxenda dose is essential to assess treatment efficacy, identify potential complications, and ensure the medication continues to provide meaningful benefit. A structured approach to monitoring supports informed decision-making about treatment continuation.
Weight and BMI tracking should occur at regular intervals. NICE TA664 recommends formal review at 12 weeks on the 3.0 mg dose to assess whether the 5% weight loss threshold has been achieved. If this target is met, treatment may continue with ongoing monitoring every 3–6 months. Weighing yourself weekly at home, at the same time of day and under similar conditions, provides useful trend data. However, remember that weight fluctuates naturally, and the overall trajectory over weeks and months is more meaningful than day-to-day variations.
Metabolic parameters warrant periodic assessment, particularly in patients with weight-related comorbidities. For those with type 2 diabetes, HbA1c monitoring helps evaluate glycaemic control improvements. Blood pressure measurements track cardiovascular benefits, whilst lipid profiles may demonstrate improvements in cholesterol levels. These metabolic improvements often continue even after weight loss plateaus, representing important health benefits beyond the number on the scales.
Realistic expectations about weight loss patterns help maintain motivation. Initial weight loss is typically more rapid during the titration phase and early maintenance period. After 3–6 months, the rate of weight loss generally slows, and many patients reach a weight plateau. This does not necessarily indicate treatment failure; maintaining weight loss represents a significant achievement given the body's natural tendency to regain weight. Research shows that patients maintaining Saxenda treatment sustain greater weight loss compared to those who discontinue.
Lifestyle factors remain crucial throughout treatment. Saxenda is licensed as an adjunct to a reduced-calorie diet and increased physical activity, not as monotherapy. Continuing to engage with dietary modifications and regular exercise maximises treatment benefits. If weight loss stalls despite good adherence to Saxenda and lifestyle measures, discuss this with your healthcare provider to explore potential contributing factors.
Treatment duration should be reviewed regularly. Whilst some patients use Saxenda for extended periods (12 months or longer), the optimal duration varies individually. Your prescriber will consider factors including weight loss achieved, metabolic improvements, tolerability, cost-effectiveness, and your personal circumstances when discussing whether to continue, adjust, or discontinue treatment. Within NHS services, eligibility for Saxenda is typically determined according to NICE TA664 criteria and local commissioning arrangements.
The standard maintenance dose of Saxenda is 3.0 mg administered once daily via subcutaneous injection. This dose is reached after a five-week titration period and is designed for long-term use throughout treatment.
Remaining on a lower maintenance dose (such as 2.4 mg or 1.8 mg) may be considered if you experience intolerable side effects at 3.0 mg, but this represents off-label use requiring discussion with your prescribing clinician and individualised clinical judgement.
According to NICE TA664, Saxenda should be discontinued if you achieve less than 5% weight loss after 12 weeks on the 3.0 mg maintenance dose. Treatment should also be stopped immediately if you become pregnant or develop severe adverse effects such as pancreatitis.
All medical content on this blog is created based on reputable, evidence-based sources and reviewed regularly for accuracy and relevance. While we strive to keep content up to date with the latest research and clinical guidelines, it is intended for general informational purposes only.
DisclaimerThis content is not a substitute for professional medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional with any medical questions or concerns. Use of the information is at your own risk, and we are not responsible for any consequences resulting from its use.